
Almost a generation of Canadian children have grown up without ever seeing a display of cigarettes in corner stores. Almost three years have passed since corner stores across Canada were required to take down promotional displays of electronic nicotine products.
And yet self-service displays of nicotine products are once again beside the cash registers across Canada. Since January, Circle K, Shell and other retailers have supported the national launch of a modernized nicotine gum sold under the brand Sesh+.
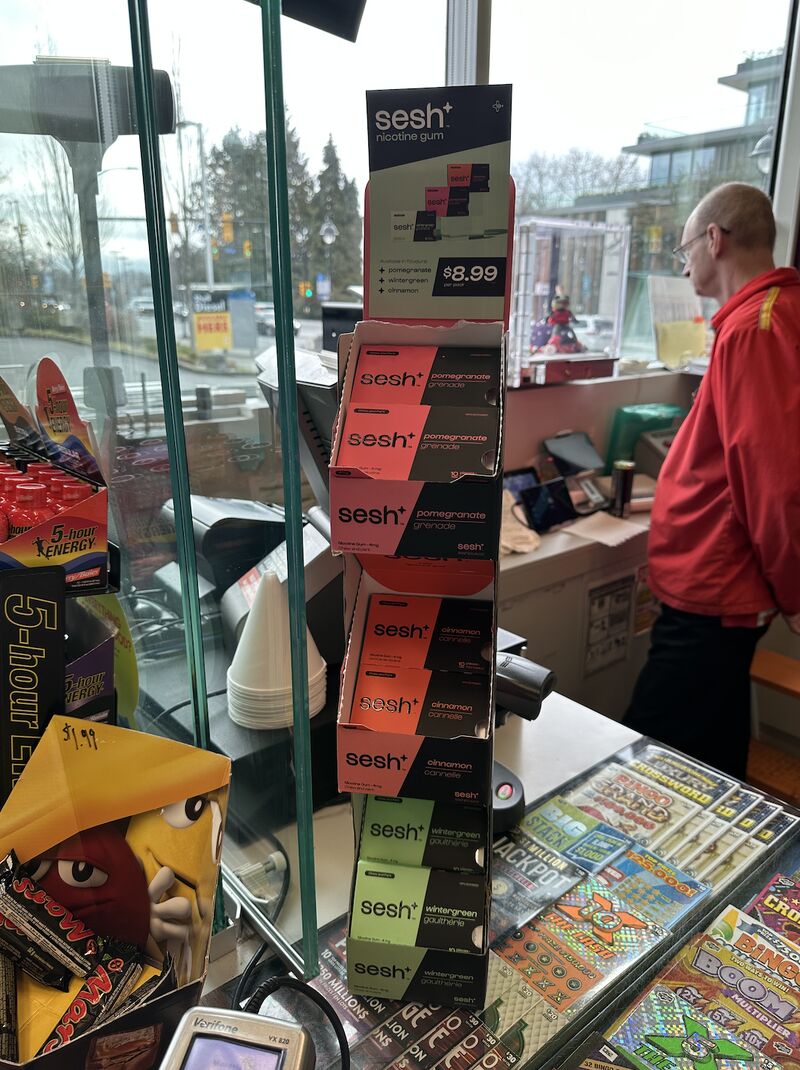 |
| Sesh+ display at Shell Station |
The federal law which governs these products does not include restrictions on paid promotional displays.
Sesh+: not your father's NRT
Sesh+ distinguishes itself from the more staid NRT manufactured by established consumer pharmaceutical companies.
- it is sold in convenience stores, not pharmacies
- it is packaged to resemble ordinary chewing gum
- the outer-labelling does not indicate that it is intended for therapeutic use
- it is sold in more exotic flavours (i.e. pomegranate)
- it is sold in smaller packages with a lower price (SRP $8.99)
Sesh+: A Canadian start-up with an American footprint.
Sesh products is owned and operated out of Vancouver, B.C. It was incorporated in Canada in November 2020 and a year later in the United States. In September 2021, the company applied to trademark its brand for both nicotine gum and pouches.
Sesh+ nicotine gum are reported to have first appeared in stores in April 2022. Sesh+ nicotine pouches are sold on-line to Canada from the United States, but are not legal for sale in stores. Sesh Products does not manufacture either Sesh+ gum or pouches, but sells gum made in the United States and pouches made in Sweden.
From the registration on Health Canada's Licensed Natural Health Products Database, it is evident that Sesh+ gum is the same as the nicotine gum sold in the United States under the Lucy brand name. They share the same Natural Product Number (NPN 80108821). The same NPN number is used on Luy Brand Spearmint, Citrus Berry and Red Mango (available online only), and on Sesh+ branded flavours cinnamon, wintergreen and pomegranate.
 |
| Sesh+ and Lucy are the same product sold in Canada different flavours under different names. They share a Natural Products number. |
Sesh+: Marketing hype or new nicotine formulations?
The Sesh+/Lucy nicotine gum is promoted as being different (and better) than Nicorette and other established brands. These marketing claims are considerably more subtle in Canada than in the U.S.
In Canada, the product is promoted by Mr. Cunningham as a product which overcomes the "negative stigma around trying to overcome addiction, the toll on mental health, and asking for support ... Sesh+ was my way of providing people with something that I knew worked, was accessible, delicious, and not something you needed to hide.”
pH Adjusters. We use a customized buffering system which interacts with the nicotine as it is released from the resinate and gum matrix in order to maximize buccal absorption. Absorption of nicotine across the buccal membrane depends on the amount of nicotine present in the unionized “free base” form. In an acidic (low) pH, nicotine is ionized and does not cross biological membranes, whereas in an alkaline (high) pH environment, nicotine is un-ionized and readily absorbed. We invested a lot of effort into ensuring that our buffering system maximizes the amount of free base nicotine while avoiding the acrid taste of standard buffer systems.
Sesh+: an offshoot from the tobacco industry
The founder and owner, Max Cunningham, is not new to the nicotine market, having once worked to promote products for Imperial Tobacco. He identifies on his LinkedIn profile that prior to working full time on Sesh+ in September 2021 he worked for Market Recon where he "created and executed marketing and sales strategies on behalf of one of the world's largest tobacco company's for their next generation product category." (Market Recon supplies retail promotions and brand activation for Imperial Tobacco).
Mr. Cunningham says his motivation for entering the business was his own addiction to vaping. “Like many young adults around the world, when vaping first hit the market, I thought it caused no real harm to my health. But shortly after I started, I felt my physical health decline specifically in my lungs and shortness of breath. Once I noticed the negative effects on my body I knew I had to quit, but after a couple of failed tries I realized it wasn’t that simple.”
Sesh+ gum: Good or bad for public Health?
(1) Walsh RA. Over-the-counter nicotine replacement therapy: a methodological review of the evidence supporting its effectiveness. Drug Alcohol Rev. 2008 Sep;27(5):529-47. doi: 10.1080/09595230802245527. PMID: 18696300.
(2) Unger JB, Barker J, Cruz TB, Leventhal AM, Pentz MA. Lucy-Novel Flavored Nicotine Gum, Lozenges, and Pouches: Are They Misleading Consumers? Subst Use Misuse. 2022;57(8):1328-1331. doi: 10.1080/10826084.2022.2076881. Epub 2022 May 19. PMID: 35586938; PMCID: PMC9451008.













{kind=link}